
by Plernta Sukjarernchaikul
When someone thinks of chilli, the first thing that they normally remember is the hot pungent taste of many cultivars, despite the fact that they have both hot and non-hot varieties. Although this plant is normally used as spices and food in several cuisines, it had historical usages as a medicinal plant in many regions around the world. Many pharmacological and clinical studies about active constituents and therapeutic benefits have been explored. Nevertheless, there are also the potential adverse reactions that have to be considered.
Introduction
Chilli is a common name for plants which are members of genus Capsicum in the Solanaceae (the potato family). There are 40 accepted species from a total of 205 species names (The Plant List, 2013). The most common and widely cultivated is C. annuum L. Other domesticated species are C. baccatuum L., C. pubescens Ruiz et Pav., C. chinese Jacq. and C. frutescens L. Chilli is one of the plants that can be found in the Medicinal Herb Spiral at Mecklenburgh Square garden. This plant is generally grown as an annual herb or subshrub in temperate regions but can be a perennial plant in tropical countries. The height can reach 150 cm (Langer and Hill, 1991). It has perfect flowers with different colours and sizes (Wahyuni et al., 2013). There are both female and male reproductive structures in the same flower which can fertilise by the process of self-pollination (Padilha and Barbieri, 2016). The fruits provide variation in length, colour and pungency depending on the species. The pigment of fruits can vary from white, purple, green or black when unripe and changes to yellow, orange or red when mature (Burt, 2005).

fig.1: Capsicum annuum in Koehler’s medicinal plants (Medizinal-Pflanzen) 1887
The main component which provides the heat / spicy sensation is capsaicin. It is produced by the specialised gland on the membrane between the fruit’s outer layers and the seeds inside a fruit (Borges, 2001). The level of pungency can be measured by the Scoville method which was developed in 1912 by dissolving dried chilli in syrup until the tester cannot detect the heat. The results are presented in Scoville Heat Units (SHU) ranging from zero to millions SHU (Hayman and Kam, 2008).

fig 2: Examples of the many varieties of ‘chilli’ (in Kantar et al 2016)
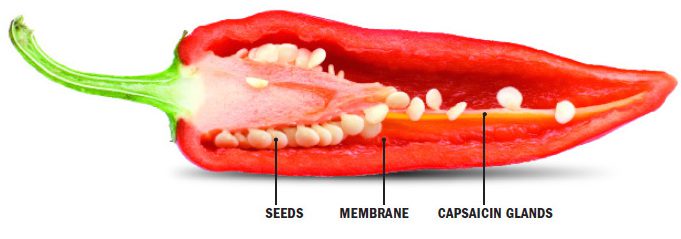
fig 3 : Morphology of the fruit of a chilli (in Dewitt 2015)
Popular history and contemporary use
Some people might think that chilli originated from Mexico because of the popularity in the country, but this plant has an origin in South America, specifically in areas of Southern Brazil and Bolivia (Nunn and Qian, 2010), and has been dispersed to many countries around the world. In 1493, Christopher Columbus took the first samples to Spain and then they were spread to other European countries (Katz, 2009) and beyond. Chillies were taken to Asian countries by a distribution of Portuguese merchants through Iran, Indonesia and India (Borges, 2001). It has been utilised in everyday life such as food, as an ornamental and in defensive sprays, as well as for its therapeutic benefits (Barceloux, 2008).
In many countries traditional uses of chilli as medicines have been recorded. In South America, people drank an infused water of chillies and honey or salt for treating cough. The infusion with sugar and cinnamon was also used for alleviating upper abdominal pain after heavy drinking of alcohol in West Indies. In England, chilli was used for the treatment of indigestion, palsy, gout, oedema and cachexia (Ainslie, 1826). African people utilised it as antiseptics for wound healing and intestinal parasitic infection. In India, the evidence was present in Sushruta Samitha, an ancient Sanskrit text on Ayurveda. Chilli with pepper, liquid amber and garlic were made into a dermal patch for decreasing the pain symptoms from gout, rheumatism and chronic lumbago or the pain in muscles and joints of the lower back. It was used for reduction of the inflammation of tonsils by preparing into a paste. Along with sugar and tragacanth, it served as a lozenge used for hoarseness. Moreover, chilli has been applied for enhancing appetite, minimising flatulence and as a remedy for cholera (Dasgupta and Fowler, 1997).
Currently, there are several commercial medical products containing chilli. Capsaicin is taken as an active ingredient in topically applied creams and patches for the treatment of pain conditions (Barceloux, 2008). In the United Kingdom, capsicum can be found in the list of herbal medicines which granted traditional herbal registration (THR) by the Medicines and Healthcare Products Regulatory Agency (MHRA) (MHRA, 2017). It is used as an active ingredient in combination with other constituents for the relief of pains, indigestion, coughs, colds and sore throats. Moreover, there are licensed pain relieving products with a Product Licence (PL) number; topical creams containing 0.025% or 0.075% of capsaicin and dermal patches with 8% capsaicin or 179 mg/patch (NICE, 2017). Many dietary supplements also add capsaicin for the potential actions to help digestion and increase fat burning rate for the people who want to lose weight.
Phytochemistry
The main active compound in chilli is capsaicin which is a colourless, odourless, lipophilic molecule. Pure capsaicin produces the high level of pungency around 15 million SHU (Wahyuni et al., 2013). Capsaicin is a chemical member in the group of capsaicinoids. Other compounds in this group are dihydrocapsaicin, nordihydrocapsaicin, homodihydrocapsaicin and homocapsaicin. Apart from capsaicinoids, there is the group of capsinoids, the capsaicinoid-like compounds, consisting of capsiate, dihydrocapsiate and nordihydrocapsiate. The differences between capsaicinoids and capsinoids are the moieties on the branched chain fatty acid and the taste. While capsaicinoids provide the pungency, capsinoids produce the heatless sensitivity.
In addition, chilli has high nutritional content of vitamin A, vitamin C, vitamin E, flavonoid and folate (Kantar et al., 2016; Wahyuni et al., 2013). Nonetheless, there is a variation in the contents depending on the species and cultivar / hybrid, maturity, cultivated regions and cooking preparation. Although the amount of nutrients which people can consume is less than from other sources, it could be a valuable source of nutrients for malnourished people living in developing countries to decrease vitamin deficiency.
Pharmacology
Many pharmacological actions of chilli have been investigated. The main medicinal benefits which have been discovered are for pain symptoms and problems associated with obesity.
The feeling of pain occurs in an area with an injury or inflammation. During the abnormal process, there is an automatic stimulation of the pain receptors which cause the release of chemicals. These chemicals bring the signals to the spinal cord and brain, which in turn processes these signals into the pain message. This communication is sent back to the injured area resulting in pain perception (Hawthorn and Redmond, 1998). One of the significant receptors that involve with the pain is transient receptor potential vanilloid 1 receptor (TRPV1), the specific neurone receptor which modulates the sensation of heat and pain.
Capsaicin has a capability to bind to the TRPV1 receptor and causes the heat sensation (Ramsey, Delling and Clapham, 2006). Besides capsaicin, TRPV1 can be stimulated by other triggers such as low pH and high temperature (>43°C), etc. Following the initial activation of the receptors, neurones are desensitised to further pain stimuli (Hayman and Kam, 2008). The mechanism of desensitisation was clarified by Sharma, Vij and Sharma (2013). They demonstrated that while TRPV1 binds to capsaicin during receptor activation, there is not only a release of neuropeptides helping to communicate the pain signals, but also an indirect depletion of neuropeptides from the neurons preventing the pain transmission as it blocks the transportation of substance P, the important peptides for a pathway of pain signals from nerves to central nervous system. Therefore, the desensitisation occurs and results as an analgesic property.
Moreover, chilli is also a well-known plant being used for a reduction of obesity due to its effects which do not only increase energy expenditure (Ludy and Mattes, 2011), but also enhances lipid oxidation (Shin and Moritani, 2007). Experiments conducted in mice (Lee et al., 2013) found that topical application of capsaicin causes an increase in the secretion of adipokines, the proteins which are produced by adipose tissue to regulate fatty acid breakdown. The results showed that mice which received capsaicin application had an improvement in lipid metabolism. Nevertheless, people could not obtain chilli in the large quantity to receive the anti-obesity effect due to its pungency. Therefore, Kawabata et al. (2009) studied this effect in non-pungent CH-19 sweet chilli and found that it provided similar effects on energy metabolism. Interestingly, this action appeared only in the mice with TRPV1 but did not occur in the TRPV1 knockout mice. Hence, the weight reduction property of chilli seems to be dependent on the TRPV1 receptor.
In addition, the potential pharmacological benefits of capsaicin for treating of numerous diseases such as cancer, cardiovascular diseases, gastrointestinal ailments, bladder syndromes and dermatological conditions have been studied. However, certain mechanisms are still unclear and detrimental effects of capsaicin on these illnesses were also reported (Sharma, Vij and Sharma, 2013). Therefore, the results of these actions are still inconsistent and further research is required.
Clinical evidence
There are many clinical trials for the usages of capsaicin, especially for the purposes of pain alleviation and weight reduction (Edwards et al. 2015).
In the pain treatment, Mason et al. (2004) conducted a meta-analysis of double-blind placebo-controlled trials to study the effectiveness of capsaicin (0.035% and 0.075%) There is the total of 1556 patients included in this review. The pain was classified into two categories. The first group was chronic musculoskeletal pain such as back pain, osteoarthritis, fibromyalgia or other chronic muscle pains. Another one was neuropathic pain ranging from post-surgical pain, diabetic neuropathy, post-herpetic neuralgia or other neuropathies. Capsaicin provided a better efficacy than placebo for both neuropathic and musculoskeletal pains. However, the result are not in agreement with the review of Derry et al. (2012) from the Cochrane library, the source of high-quality evidence for scientific research, who studied the effects of capsaicin on chronic neuropathic pain focusing on lower concentrations (<1%). The small size of studies probably resulted in a bias and, in conclusion, capsaicin was unlikely to provide significant effect further than compared to placebo creams. In contrast, the Cochrane review of the high concentration (Derry et al., 2017) concluded that the patches containing a high concentration of capsaicin (8%) in a single application could give a moderate or substantial pain relief better than the control.
The clinical studies of capsaicin for weight management of Janssens, Hursel and Westerterp-plantenga (2014) suggested that 2.56 mg of capsaicin added to the meal could increase the feeling of fullness in energy balance and prevent the effects of negative energy balance on the desire to eat after mealtime. Similarly, Whiting, Derbyshire and Tiwari (2014) reported that capsaicin consumption before the meal resulted in a decrease of energy intake around 74 kcal and suggested at least 2 mg of capsaicin prior to the meal for this outcome. In addition, Ludy and Mattes (2011) recommended consuming chillies by oral ingestion rather than in capsule form to achieve the maximum benefit.
Toxicity and Side Effects
The general adverse effects of topical capsaicin are redness and burning. These have become the major limitations of utilising chilli as a medication and turn out to be critical problems of the tests as blinding the experiments is not possible and cause the withdrawal of volunteers (Derry et al., 2012; Ludy and Mattes, 2011). Moreover, capsaicin exposure could lead to high irritation as can be seen from pepper spray usage. Getting into eyes can cause tearing, blepharospasm and conjunctivitis. Over-consumption may result in nausea, vomiting, abdominal pain and burning diarrhoea (Hayman and Kam, 2008).
However, capsaicin is considered as a safe compound which has been used as a cough-inducer in many experiments for the cough challenge testing of antitussive medicines (Dicpinigaitis, 2012). It is also asserted that there is no detrimental consequence occurred in more than 90% of the studies (Dicpinigaitis and Alva, 1984). Although these reports show chilli to be harmless, these studies have been using limited amounts and under the supervision of specialists. Therefore, the usage of capsaicin should be determined for an appropriate amount to avoid adverse effects that might occur.
Conclusion
Chilli is not only a popular plant as part of many diets and cuisines, but it also provides pharmacological benefits. Modern scientific studies have demonstrated its effects on several diseases, especially for the pain and weight reduction. For an alleviation of pain symptom, while a low concentration (<1%) seems to be unable to contribute to a decrease in neuropathic pains, a single application of high concentrated capsaicin (8%) could significantly enhance recovery from painful conditions. In addition, the oral consumption of around 2mg capsaicin has an important role in weight management. However, although capsaicin is marked as a safe compound for scientific experiments, it can cause irritation if there is excessive consumption or exposure. Therefore, to avoid side effects with medical uses, users have to follow the instructions on a label or the recommendation of a doctor.
Disclaimer
In this essay, we do not intend to advise or recommend herbs for medicinal or health use. This information is for educational purposes only and should not be considered as a recommendation or an endorsement of any particular medical or health treatment. The use of any such products should be based on the appropriate advice of a health care professional or based on the information available in the patient information leaflets (i.e. for THR products). The information provided should not be used during any medical emergency or for the diagnosis or treatment of any medical condition.
© Plernta Sukjarernchaikul 2017
Plernta Sukjarernchaikul, MSc student in Medicinal Natural Products and Phytochemistry at the UCL School of Pharmacy, University College London
MSc student (2016-2017), Research Cluster ‘Biodiversity and Medicines’ /
Centre for Pharmacognosy and Phytotherapy,
UCL School of Pharmacy, Univ. London
29-39 Brunswick Sq., LondonWC1N 1AX
References
Ainslie, W., 1826. Materia Indica; Or, Some Account of Those Articles which are Employed by the Hindoos and Other Eastern Nations, in Their Medicine, Arts, and Agriculture. Longman, Rees, Orme, Brown, and Green.
Barceloux, D.G., 2008. Pepper and Capsaicin (Capsicum and Piper Species). Medical Toxicology of Natural Substances: Foods, Fungi, Medicinal Herbs, Plants, and Venomous Animals, pp.71–76.
Borges, R.M., 2001. Why are chillies pungent? Journal of biosciences, 26(3), pp.289–291.
Burt, J., 2005. Growing capsicums and chillies. Development of Agriculture and Food, (64).
Dasgupta, P. and Fowler, C.J., 1997. Chillies: from antiquity to urology. British journal of urology, 80(6), pp.845–852.
Derry, S., Ra, M., Derry, S., Ra, M., Derry, S. and Moore, R.A., 2012. Topical capsaicin (low concentration) for chronic neuropathic pain in adults. (9).
Derry, S., Rice, A.S.C., Cole, P., Tan, T. and Moore, R.A., 2017. Topical capsaicin (high concentration) for chronic neuropathic pain in adults. The Cochrane Library, (1).
Dicpinigaitis, P. V, 2012. Effect of drugs on human cough reflex sensitivity to inhaled capsaicin. Cough, 8(1), p.10.
Dicpinigaitis, P. V and Alva, R. V, 1984. Safety of Capsaicin Cough Challenge Testing. CHEST, 128(1), pp.196–202.
Edwards, S., Costa-Rocha I. da, Williamson E.M., Heinrich, M. 2015 Phytopharmacy – an evidence-based guide to herbal medicines. Wiley, Chichester.
Hawthorn, J. and Redmond, K., 1998. Pain: Causes and Management. Malden, Mass: John Wiley and Sons, Inc.
Hayman, M. and Kam, P.C.A., 2008. Capsaicin: A review of its pharmacology and clinical applications. Current Anaesthesia & Critical Care, 19(5), pp.338–343.
Janssens, P.L.H.R., Hursel, R. and Westerterp-plantenga, M.S., 2014. Capsaicin increases sensation of fullness in energy balance , and decreases desire to eat after dinner in negative energy balance. Appetite, 77, pp.44–49.
Kantar, M.B., Anderson, J.E., Lucht, S.A., Mercer, K., Bernau, V., Case, K.A., Le, N.C., Frederiksen, M.K., Dekeyser, H.C., Wong, Z., Hastings, J.C. and Baumler, D.J., 2016. Vitamin Variation in Capsicum Spp. Provides Opportunities to Improve Nutritional Value of Human Diets. PloS one, 11(8), pp.1–12.
Katz, E., 2009. Chili Pepper, from Mexico to Europe: Food, Imaginary and Cultural Identity. Food, Imaginaries and Cultural Frontiers. Essays in honour of Helen Macbeth, Guadalajara, Universidad de Guadalajara, Colección Estudios del Hombre, Serie Antropología de la Alimentación, pp.213–232.
Kawabata, F., Inoue, N., Masamoto, Y., Kimura, W., Kadowaki, M., Higashi, T., Tominaga, M., Inoue, K., Fushiki, T., Noue, K.I. and Ushiki, T.F., 2009. Non-Pungent Capsaicin Analogs (Capsinoids) Increase Metabolic Rate and Enhance Thermogenesis via Gastrointestinal TRPV1 in Mice. Bioscience, biotechnology, and biochemistry, 73(12), p.2690=2697.
Langer, R.H.M. and Hill, G.D., 1991. Solanaceae. In: Agricultural plants. Cambridge University Press,
pp.308–327.
Lee, G., Shin, M.K., Yoon, D., Kim, A., Yu, R., Park, N. and Han, I., 2013. Topical Application of Capsaicin Reduces Visceral Adipose Fat by Affecting Adipokine Levels in High-Fat Diet-Induced Obese Mice. Obesity, 21(1), pp.115–122.
Ludy, M. and Mattes, R.D., 2011. The effects of hedonically acceptable red pepper doses on thermogenesis and appetite. Physiology & Behavior, 102(3), pp.251–258.
Mason, L., Moore, R.A., Derry, S., Edwards, J.E. and Mcquay, H.J., 2004. Systematic review of topical capsaicin for the treatment of chronic pain. Bmj, 328(7446), pp.1–5.
MHRA, 2017. Herbal medicines granted a traditional herbal registration (THR). [online] Available at: <https://www.gov.uk/government/publications/herbal-medicines-granted-a-traditional-herbal-registration-thr/herbal-medicines-granted-a-traditional-herbal-registration> [Accessed 20 Mar. 2017].
NICE, 2017. Drugs for the treatment of soft-tissue disorders and topical pain relief. [online] Available at: <https://www.evidence.nhs.uk/formulary/bnf/current/10-musculoskeletal-and-joint-diseases/103-drugs-for-the-treatment-of-soft-tissue-disorders-and-topical-pain-relief> [Accessed 21 Mar. 2017].
Nunn, N. and Qian, N., 2010. The Columbian Exchange: A History of Disease, Food, and Ideas. The Journal of Economic Perspectives, 24(2), pp.163–188.
Padilha, H.K.M. and Barbieri, R.L., 2016. Plant breeding of chili peppers (Capsicum , Solanaceae) – A review. Australian Journal of Basic and Applied Sciences, 10(15), pp.148–154.
Ramsey, I.S., Delling, M. and Clapham, D.E., 2006. An introduction to TRP channels. Annu. Rev. Physiol., 68, pp.619–647.
Sharma, S.K., Vij, A.S. and Sharma, M., 2013. Mechanisms and clinical uses of capsaicin. European Journal of Pharmacology, 720(1), pp.55–62.
Shin, K.O. and Moritani, T., 2007. Alterations of Autonomic Nervous Activity and Energy Metabolism by Capsaicin Ingestion during Aerobic Exercise in Healthy Men. Journal of nutritional science and vitaminology, 53(2), pp.124–132.
The Plant List, 2013. Capsicum. [online] Available at: <http://www.theplantlist.org/1.1/browse/A/Solanaceae/Capsicum/> [Accessed 1 Jun. 2017].
Wahyuni, Y., Ballester, A., Sudarmonowati, E., Bino, R.J. and Bovy, A.G., 2013. Secondary Metabolites of Capsicum Species and Their Importance in the Human Diet. Journal of natural products, 76(4), pp.783–793.
Whiting, S., Derbyshire, E.J. and Tiwari, B., 2014. Could capsaicinoids help to support weight management? A systematic review and meta-analysis of energy intake data. APPETITE, 73, pp.183–188.
Figure Credits
Figure 1: Source: Köhler, F.E., 1887. Ilustración de los caracteres de la especie Capsicum annuum: A. Muestra de un espécimen en flor (a tamaño natural). [online] Available at: <https://commons.wikimedia.org/wiki/Capsicum_annuum#/media/File:Illustration_Capsicum_annuum0.jpg> [Accessed 19 Mar. 2017].
Figure 2: Source: Kantar, M.B., Anderson, J.E., Lucht, S.A., Mercer, K., Bernau, V., Case, K.A., Le, N.C., Frederiksen, M.K., Dekeyser, H.C., Wong, Z., Hastings, J.C. and Baumler, D.J., 2016. Vitamin Variation in Capsicum Spp. Provides Opportunities to Improve Nutritional Value of Human Diets. PloS one, 11(8), pp.1–12.
Figure 3: Source: Dewitt, D., 2015. Did we humans coevolve with chile peppers and marijuana? [online] Available at: <http://www.dave-dewitt.com/2015/11/19/did-we-humans-coevolve-with-chile-peppers-and-marijuana/> [Accessed 20 Mar. 2017].